What is Overpronation?
If you've been told you overpronate, you may have been left asking the question: What is overpronation?. This article aims to both answer that question and challenge much of what the running shoe industry has been trying to sell us on for many years!
Overpronation is described as an excessive amount of pronation (inward collapse of the foot) during the weight bearing phase of walking and running gait. It is often claimed that overpronation can cause injury in runners.
However in this article, I'll be putting those claims under some close scrutiny.
I've written this article specifically to discuss some of the research that guides what we know about pronation of the foot, and in doing so facilitate the conclusion that the term “overpronation” is neither accurate, descriptive nor meaningful.
What is Pronation of the Foot?
Pronation of the foot is simply a description of a normal joint movement. Whilst this article is referring to this motion in the lower limb, it is worth remembering that pronation is not isolated to the lower limb; the upper limb can of course also pronate - this occurs at the distal radioulnar joint in the wrist (when checking your watch to see what the time is for example).
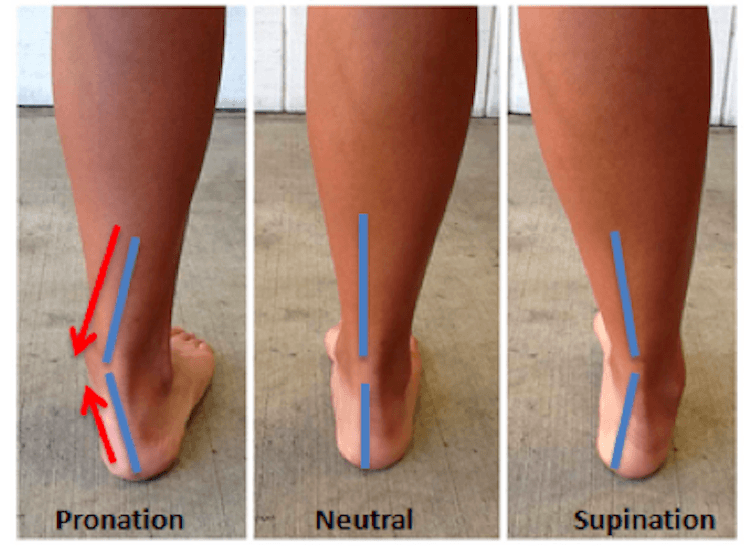
Pronation of the foot is seen as a combination of abduction, eversion and dorsiflexion (when weight-bearing) and this motion occurs primarily at the subtalar joint, which is the articulation between the talus and the calcaneum (heel bone).
Here's a very short video to show the difference in foot posture between pronation and supination:
How Much Pronation is Normal?
The theoretically conceived reference for an ‘ideal foot’ is essentially still what many modern-day biomechanical evaluations and management plans are dependent upon despite the fact that this paradigm was first introduced in the early 1970’s.
Feet which did not fit stated criteria were deemed as ‘abnormal’ with the assumption being that they may be less efficient and more prone to injury due to compensations which may occur during activity.
Somewhere along the line, this information evolved into what became the cornerstone of most educational programmes on foot function; that we should function either in, or very close to subtalar joint neutral (the position when the subtalar joint is neither pronated nor supinated).
It should be noted that this has never been suggested in any research, instead just gaining popularity within both medical and lay communities insidiously.
Studies have shown that the structural anatomy of the human subtalar joint varies from person to person and it has also been shown that the location of the axis of the joint can and does vary from person to person; this will of course directly influence the magnitude of foot pronation and supination seen.
In light of this sort of evidence, it seems odd that there would be an expectation that all individuals could or should function similarly or identically.
Across many studies, all of the data collected from pain-free and injury-free subjects and athletes shows that very few individuals actually meet the historical definition of ‘normal’.
One study examined 120 healthy individuals both non-weight bearing and weight bearing. Not one subject conformed to the historical criteria of a ‘normal’ foot.
Further searching through the literature shows that the majority of data collected from sampled populations suggests that the normal (average) foot position at rest is actually mildly to moderately pronated, as opposed to ‘neutral’.
How is pronation of the foot measured?
Considering the many different ways to quantify foot level pronation, there is actually no agreement on the best way of examining static subtalar joint pronation. Clinical measurement of foot position is renowned for being challenging due to the complex interactions of the many joints involved.
What is clear is that irrespective of the measurement method chosen, the reliability of such measurements is found to be poor to moderate, at best.
With respect to finding the subtalar joint neutral position, even experienced Podiatrists are only within 3o of subtalar joint neutral 90% of the time as shown by a Canadian study.
Another issue to consider with static measurements of pronation is that there is some disagreement as to whether they are associated with dynamic foot function, with growing evidence that there is little to no relationship between the two.
Indeed many podiatrists have ceased clinically quantifying these measurements for all of these reasons.
Injuries Caused by Pronation of the Foot
It is a commonly held belief that pronation will increase the risk of lower extremity injury. However (perhaps surprisingly) this is not particularly well supported by the literature, with very few studies which actually show pronation of the foot increases injury risk.
Instead, there are numerous pieces of work which have shown there is no association with foot type and injury and some research exists which even suggests that a pronated foot type is actually protective against injury. This is not to say that some individuals will not suffer from pain or discomfort which may be associated with their foot motions or pronation patterns.
What is certainly clear, however, is that the relationship between pronation and injury is poorly understood at this time and is far from consistent or predictable.
Summary
The available research on pronation of the foot points to the following conclusions:
- It is difficult to accurately and repeatably measure foot level pronation
- The relationship between pronation and injury is very poorly understood
- The historical concept of ‘normal’ is erroneous
- Variation between people in foot level movement patterns is high (and this is normal)
Challenging the Myth of Overpronation
Here's an interview I recorded a little while ago where I go into much more detail about the issues with the term "overpronation":
What does this mean for Overpronation?
Overpronation is often used to describe a foot which is in a pronated position, but considered to be ‘too pronated’ or ‘more pronated than normal’. It is also generally referred to in a negative way, in that it will often be considered to be pathological and in need of ‘correction’. It is even used by some as a diagnosis.
Ambiguity
A golfer has just hit a shot 150 yards. Have they “over” hit it? To correctly answer that question you would need to know exactly how far they were supposed to hit it or what they were aiming for...
In order to be able to confidently state that something is happening too much, then by definition we must be comparing it to how much it should happen. Hopefully what has become clear by now is that we do not know how much pronation is ‘normal’. All we do know that it will likely be different from person to person (and of course activity to activity). Essentially, we do not necessarily know what we are aiming for in a given individual, so how can we say when it is “over”?
Pronation used as a Diagnosis
In addition to the now obvious ambiguity of the term, the use of "pronation" or worse "overpronation" as a diagnosis is most certainly to be discouraged. Many individuals present to my clinic with the information that they have been previously diagnosed as an “overpronator”.
As mentioned earlier, pronation is simply a motion – an observation, but never a diagnosis. Imagine two different athletes present with feet which appear to function in a similar manner, and it is noted they are both in a maximally pronated position.
Athlete 1 complains of pain on the inside of the ankle.
Athlete 2 complains of pain on the outside of the ankle.
How could they both be diagnosed with the same “condition”? Grouping all foot and ankle pains into one convenient ‘diagnosis’ is at best ill-informed, and at worst is delivering a care below the standard of that which athletes deserve.
Pronation used as a Scapegoat
The majority of athletes presenting to sports injury clinics across the globe will already be injured. As the aforementioned research has shown, normative data suggests that most individuals have a mild to moderately pronated foot type (rather than a neutral alignment which is erroneously thought to be ‘normal’).
Therefore whilst it has often been assumed that foot posture may be one of the contributing factors in a presenting lower limb injury (which of course it may well be for some), the subtle differences between causation and correlation should always be kept in mind.
Just because a foot/lower limb which hurts is pronated, does not mean that it hurts because it is pronated. This is why a thorough history of the mechanism of the presenting injury and all other potential contributing factors are just as important as foot posture, and should be concurrently investigated.

Overpronation and management of injury
So, can idetifying “overpronation” help formulate treatment plans for injured individuals? In the fictitious athletes mentioned above, how does classifying or terming them to be “overpronating” guide a clinician in treating them?
It could be argued that doing so and treating them both in a similar manner (increasing subtalar joint supination moments for example) may achieve a desirable result.
However looking at a foot position, attaching a vague and meaningless term to it, and then initiating a blanket management plan which seems to be the same irrespective of the exact problem is very bad science at best, and at worst could be considered grossly negligent.
So, if not Overpronation, then what?
A fair question may be that if we are to abandon the term “overpronation” then what do we use in is place? The answer to this is: nothing.
Hopefully, it is now clear that Overpronation is a term which contributes nothing to our understanding – it is not definable, not reliable or valid, not diagnostic, its relationship to injury is not fully understood, and it does not dictate what the most appropriate management plan may be. It should not be replaced, it should be removed.
A more appropriate way to move forward with respect to assessing and treating injured individuals is to accurately identify the injured anatomical structure (formulate a diagnosis), identify the structural and functional characteristics of the foot and lower extremity, determine the most likely type of tissue stress which is causing the pathology, and then design the management plan to reduce these stresses and optimise gait function accordingly.
Image of the ankle by Ducky2315 [CC BY-SA 3.0]
via Wikimedia Commons
{kind=link}